科研进展
规范成人心脏骤停后综合征管理,推动复苏中心建设
谢熙 1,2 桑文涛 1 徐峰 1 陈玉国 1
1 山东大学齐鲁医院急诊科 山东省急危重症临床医学研究中心,济南 250012;
2 山东省妇幼保健院重症医学科,济南 250000
通信作者:徐峰;陈玉国
---------------------------------------------------------------------------------------------------------------
据国际复苏联盟最新报告,全球范围内院外心脏骤停(out-of-hospital cardiac arrest, OHCA)发病率不同,年发病率在(30.0~97.1)/10 万人之间 [1] ;接受救治的 OHCA患者自主循环恢复(return of spontaneous circulation, ROSC)比例约为 29.7%,但存活出院的比例仅为 8.8%[2]。这一差异来源于OHCA后机体经历的一系列病理改变,该特殊的病理生理过程最早由Vladimir Negovsky 教授在20世纪70年代报道,2008年国际上形成共识将其统一命名为心脏骤停后综合征(post-cardiac arrest syndrome, PCAS)[3],包括 :⑴心脏骤停后脑损伤 ;⑵心脏骤停后心肌功能障碍 ;⑶全身缺血 - 再灌注反应 ;⑷持续的病理生理反应(即导致心脏骤停的疾病或损伤以及潜在疾病的病理生理改变)[4]。PCAS 严重程度取决于心脏骤停的诱发因素、心脏骤停前患者的健康状况、ROSC 恢复的时间以及潜在的共患病等 [5]。
2010年更新的《美国心脏协会心肺复苏和心血管急救指南》将“生存链”增加第五个环节即心肺复苏后综合治疗 [6],针对 PCAS 提出改善组织器官灌注、治疗原发病、预防再发心脏骤停等治疗措施。2020 年《美国心脏协会心肺复苏和心血管急救指南》[7] 更新时再次强调,复苏后治疗是“生存链” 的重要一环,并建议通过全面的、结构化的、多学科的合作以实现最佳的治疗效果。参考 2020 年国际复苏联络委员会国际共识——心肺复苏和心血管急救治疗建议 [8],欧洲复苏委员会和欧洲重症监护医学学会于 2021 年更新了《复苏后治疗指南》[9]。为指导和规范我国临床医师对 PCAS 的诊疗,我国急诊领域的专家结合国内外相关指南及我国实际情况,于2021年撰写并发表了《成人心脏骤停后综合征的诊断和治疗中国急诊专家共识》[10]。目前国内外对于 PCAS 的总体治疗原则主要是 基于 PCAS 的病理生理机制,识别和治疗心脏骤停病因、预防再发心脏骤停,减少心脏骤停后继发性脏器功能损伤,预后评估及康复治疗等。本文将从以下方面对 PCAS 的治疗进行阐述。
1、复苏中心(心脏骤停中心)
加强复苏后治疗可提高心脏骤停患者的存活率 [11-12]。目前国外已开展了心脏骤停中心的建设和认证工作 [13],旨在对心脏骤停患者进行综合的复苏后治疗,改善患者预后。一项评估心脏骤停中心对 OHCA 患者远期预后影响的研究表明,患者入住心脏骤停中心接受治疗可降低死亡风险,且对于在非心脏骤停中心首诊的患者,早期转移至心脏骤停中心也可降低死亡风险 [14]。故目前国内外均建议,对于 ROSC 患者尽快入住专业的心脏骤停中心进行综合的复苏后监护治疗。
2、气道管理和呼吸支持
根据患者心脏骤停时的发病及救治情况,大多 数患者可能在心脏骤停发生前、抢救期间或 ROSC 后需要行气管插管及机械通气 [15-16]。目前研究表明,给予更多的氧可以增加大脑供氧,但较高的氧暴露反而会导致线粒体来源的活性氧增加从而加重氧化损伤 [17-18]。动物实验研究表明,与低氧浓度相比,100% 氧疗与更差的神经系统结果相关 [19]。一项对缺氧缺血性脑损伤机械通气患者保守氧疗与普通氧疗的随机对照试验结果表明,低氧目标组患者的病死率较低 [20],需要注意的是,考虑伦理学问题,本研究监测的指标是正常氧合而不是高氧血症。因此目前国内外指南建议,ROSC 患者初始使用 100%(或最大可用)吸入氧体积分数,一旦能够 可靠监测外周血氧饱和度(peripheral blood oxygen saturation, SpO2),动态调整吸入氧体积分数,使目标 SpO2 在 92%~98%,避免高氧血症和低氧血症。
动脉血二氧化碳分压(partial pressure of arterial carbon dioxide, PaCO2)升高可增加脑血流量及血容量,增加脑水肿风险,而低碳酸血症可能引起血管收缩,导致脑缺血,由此可见,PaCO2 可通过改变脑血流从而影响脑损伤后的临床结局 [21]。目前研究结果表明,暴露于低碳酸血症和高碳酸血症均与较差的临床结局相关 [22-23],但目前对于心脏骤停后与良好神经功能预后相关的最佳 PaCO2 范围仍不清楚,仍需进一步研究。因此,目前国内外指南均建议对于 ROSC 后仍处于昏迷的患者,将 PaCO2 维持在正常生理范围内(35~45 mmHg,1 mmHg=0.133 kPa)。
3、血流动力学监测及管理
约 60% 的 ROSC 患者可能出现心肌功能障碍和(或)心脏指数降低,心功能受损在 ROSC 后的 24~48 h 内比较常见,之后逐渐消失 [24]。早期超声心动图可以识别潜在的心脏病理改变,量化心肌功能障碍的程度,并帮助指导血流动力学管理 [25] ;有创血流动力学监测可量化心肌功能障碍并显示趋势 [26]。因此建议尽早、尽快对 ROSC 患者进行超声心动图检查,发现潜在的心脏病理改变并量化心肌功能障碍的程度;通过动脉导管进行持续有创血压监测,对血流动力学不稳定的患者持续监测心排血量。
目前尚无最佳目标血压,但有研究表明 ROSC 后低血压与患者不良预后相关 [27]。因此,目前国内外建议ROSC 患者应避免低血压,保持收缩压≥ 90mmHg,平均动脉压≥ 65 mmHg ;临床实践中可结合组织灌注指标,如尿量、乳酸清除率等 [28-30],对 ROSC 患者目标血压进行动态调整。去甲肾上腺素是最常用的升压药物 [31],对于 ROSC 后存在心肌功能障碍的患者,多巴酚丁胺是最常用的正性肌力药物 [32]。目前尚无指导 ROSC 后患者的最佳液体治疗方案。研究表明,在对 ROSC 后患者进行早期复苏过程中,优先使用液体复苏比血管加压药可实现更高的 MAP,并与更高的出院存活率相关 [33]。因此建议对血流动力学不稳定的患者行个体化的、综合的血流动力学评估方案指导治疗。10%~15% 的 OHCA 患者最终需要机械循环支持 [34],故对于液体复苏、血管活性药物治疗效果差(如仍持续休克)的患者,可考虑应用机械循环支持(如主动脉内球囊反搏、左心室辅助装置或动静脉体外膜肺氧合)[35]。
4、目标温度管理(target temperature management, TTM)
TTM 可减少内皮细胞激活,减轻全身炎症反应 [36-37],还可以降低谷氨酰胺和谷氨酸水平,减少继发性脑细胞死亡 [38],因此,TTM 可减轻 PCAS 脑损伤。研究表明,TTM 期间的目标温度及其持续时间对 OHCA 患者的存活率的影响,差异无统计学意义 [39],但 TTM 后的发热,提示患者预后较差 [40]。目前国内外均建议,对于 ROSC 后仍处于昏迷状态的患者可实施 TTM,将目标核心体温保持在 32~36 ℃的恒定值至少 24 h,且 ROSC 后至少 72 h 内避免发热。
5、控制癫痫发作
入住重症监护病房的心脏骤停患者中,有 20%~30% 发生癫痫,这通常是严重缺血缺氧性脑损伤的标志 [41]。癫痫发作可能会增加脑代谢,并有可能加重心脏骤停引起的脑损伤。但目前有研究表明,肌阵挛合并癫痫样放电可能是 Lance-Adams 综合征的早期症状,而这一表现与觉醒是一致的,提示良好神经功能预后 [42],如果在这种情况下, 积极的抗癫痫治疗可能影响对患者的预后评估。因此,目前国内外指南建议,对 ROSC 后仍昏迷的患者及时完善脑电图(electroencephalography, EEG)检查,明确是否存在癫痫发作,必要时动态监测 EEG ;同时不建议给予预防性抗癫痫治疗, 如出现癫痫发作,可予以药物治疗,药物选择与其他病因引起癫痫发作的治疗方案一致。
6、冠状动脉造影(coronary angiography, CAG)与血运重建
OHCA 病因以心源性疾病为主,其中冠状动脉疾病在心源性因素中很常见 [43-44]。ROSC 后患者行早期 CAG 与更高的存活出院及良好神经功能预后比率相关,且 CAG 后成功行血运重建与中期生存率提高相关 [45-46]。目前临床实践中的主要挑战是在所有 ROSC 后患者中确定 CAG 的最佳受益人群。目前国内外指南建议,ROSC 后患者应尽快完善12 导联心电图(electrocardiograph, ECG),确定是否存在急性 ST 段抬高型心肌梗死。对所有怀疑由心源性病因导致的心脏骤停且 ECG 提示 ST 段抬高的患者均应行急诊 CAG,如有需要应立即进行血运重建。而对于 ECG 提示为非 ST 段抬高的心脏骤停患者,ST 段抬高的缺失并不能完全排除近期冠状动脉闭塞 [47],因此对于 ROSC 后 ECG 提示为非 ST 段抬高的成年心脏骤停患者,早期是否行急诊 CAG 应该基于多种因素,包括既往病史、骤停前症状、首次监测心律、临床症状、超声心动图等。
7、预后评估
ROSC 后仍昏迷的患者,约有三分之二的死亡是由缺血缺氧性脑损伤引起的 [48],其中大多数脑损伤导致的死亡是由于停止生命维持治疗 (withdrawal of life-sustaining therapy, WLST)导致的 [49]。因此,对于 ROSC 后仍处于昏迷的患者进行准确的预后评估至关重要,不仅可以避免对有机会获得神经功能恢复的患者过早的做出 WLST,还可避免对存在严重和不可逆转的神经损伤患者进行无效治疗。目前仍未有特异度为 100% 的神经功能预后评估方案,因此,国际上建议一种基于临床的多模态神经预后评估策略 :(1) 评估方式,采用多模式方法进行,包括临床表现、神经电生理、生物标志物及影像学,而不是基于任何单一的发现 ;(2) 评估时间,将神经预后延迟到足够的时间,以确保避免在损伤后早期被药物作用或短暂的不良检查结果所混淆 ;(3) 评估人员,建议治疗团队与患者家属就预期的时间过程和神经预后的不确定性进行定期和透明的多学科讨论。
8、康复治疗
心脏骤停幸存者常经历一系列生理、神经、认知、情感或社会问题,其中一些可能要到出院后才会出现 [50-53]。心脏骤停后的存活是一个康复和恢复的过程,为提高心脏骤停患者远期预后,2020 年《美国心脏协会心肺复苏和心血管急救指南》[7] 的更新在“生存链”中增加了康复治疗这一环节,建议出院前对心脏骤停幸存者进行综合评估,以确定早期康复需要,并在必要时安排康复治疗。
9、总结与展望
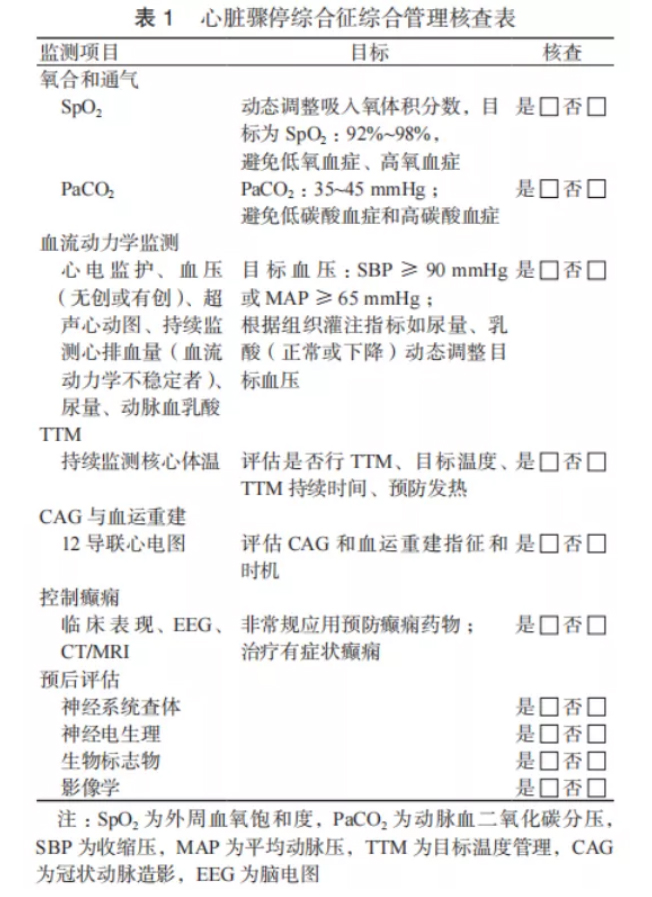
综上所述,深入认识 PCAS 的病理生理机制,并对其进行包括气道管理与呼吸支持、血流动力学监测与管理、TTM、CAG 与血运重建、预后评估、康复等在内的综合管理方案(表 1),可改善心脏骤停患者的预后。但也应清楚认识到,并非所有医院都具备提供上述高质量复苏后综合管理所需的资源和经验,因此未来可能需要多方面共同努力,结合国际先进经验,探索建设符合我国国情的复苏中心(心脏骤停中心),切实提高心脏骤停患者的存活率。
利益冲突 所有作者声明无利益冲突
参考文献
[1] Kiguchi T, Okubo M, Nishiyama C, et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR)[J]. Resuscitation, 2020, 152: 39-49. DOI:10.1016/j.resuscitation.2020.02.044.
[2] Yan SJ, Gan Y, Jiang N, et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis[J]. Crit Care, 2020, 24(1): 61. DOI:10.1186/s13054-020-2773-2.
[3] Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A scientific statement from the international liaison committee on resuscitation; the American Heart Association emergency cardiovascular care committee; the council on cardiovascular surgery and anesthesia; the council on cardiopulmonary, perioperative, and critical care; the council on clinical cardiology; the council on stroke[J]. Resuscitation, 2008, 79(3): 350-379. DOI:10.1016/ j.resuscitation.2008.09.017.
[4] Topjian AA, de Caen A, Wainwright MS, et al. Pediatric postcardiac arrest care: A scientific statement from the American Heart Association[J]. Circulation, 2019, 140(6): e194-e233. DOI:10.1161/ CIR.0000000000000697.
[5] Kang Y. Management of post-cardiac arrest syndrome[J]. Acute Crit Care, 2019, 34(3): 173-178. DOI:10.4266/acc.2019.00654.
[6] Hazinski MF, Nolan JP, Billi JE, et al. Part 1: Executive summary: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations[J]. Circulation, 2010, 122(16 Suppl 2): S250-S275. DOI:10.1161/CIRCULATIONAHA.110.970897.
[7] Merchant RM, Topjian AA, Panchal AR, et al. Part 1: Executive summary: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care[J]. Circulation, 2020, 142(16_suppl_2): S337-S357. DOI:10.1161/ cir.0000000000000918.
[8] Nolan JP, Maconochie I, Soar J, et al. Executive summary 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations[J]. Resuscitation, 2020, 156: A1-A22. DOI:10.1016/ j.resuscitation.2020.09.009.
[9] Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care[J]. Intensive Care Med, 2021, 47(4): 369- 421. DOI:10.1007/s00134-021-06368-4.
[10] 中华医学会急诊医学分会复苏学组 , 中国医药教育协会急诊专 业委员会 , 成人心脏骤停后综合征诊断和治疗中国急诊专家共 识组 . 成人心脏骤停后综合征诊断和治疗中国急诊专家共识 [J]. 中华急诊医学杂志 , 2021, 30(7): 799-808. DOI:10.3760/cma. j.issn.1671-0282.2021.07.002.
[11] Girotra S, Nallamothu BK, Tang YY, et al. Association of hospitallevel acute resuscitation and postresuscitation survival with overall risk-standardized survival to discharge for in-hospital cardiac arrest[J]. JAMA Netw Open, 2020, 3(7): e2010403. DOI:10.1001/ jamanetworkopen.2020.10403.
[12] 朱建良 , 朱建军 , 刘励军 . 心脏骤停后综合征患者早期集 束化治疗进展 [J]. 中华急诊医学杂志 , 2019, 28(1): 7-13. DOI:10.3760/cma.j.issn.1671-0282.2019.01.003.
[13] Rott N, Scholz KH, Busch HJ, et al. Criteria for the certifification of cardiac arrest centers in Germany[J]. Resuscitation, 2021, 169: 1-3. DOI:10.1016/j.resuscitation.2021.09.034.
[14] Elmer J, Callaway CW, Chang CH, et al. Long-term outcomes of outof-hospital cardiac arrest care at regionalized centers[J]. Ann Emerg Med, 2019, 73(1): 29-39. DOI:10.1016/j.annemergmed.2018.05.018.
[15] Berg KM, Grossestreuer AV, Uber A, et al. Intubation is not a marker for coma after in-hospital cardiac arrest: A retrospective study[J]. Resuscitation, 2017, 119: 18-20. DOI:10.1016/ j.resuscitation.2017.07.024.
[16] Benger JR, Kirby K, Black S, et al. Effect of a strategy of a supraglottic airway device vs tracheal intubation during out-ofhospital cardiac arrest on functional outcome: the AIRWAYS-2 randomized clinical trial[J]. JAMA, 2018, 320(8): 779-791. DOI:10.1001/jama.2018.11597.
[17] Sekhon MS, Ainslie PN, Griesdale DE. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: A “two-hit” model[J]. Crit Care, 2017, 21(1): 90. DOI:10.1186/s13054-017-1670-9.
[18] Marquez AM, Morgan RW, Ko T, et al. Oxygen exposure during cardiopulmonary resuscitation is associated with cerebral oxidative injury in a randomized, blinded, controlled, preclinical trial[J]. J Am Heart Assoc, 2020, 9(9): e015032. DOI:10.1161/JAHA.119.015032.
[19] Pilcher J, Weatherall M, Shirtcliffffe P, et al. The effffect of hyperoxia following cardiac arrest - A systematic review and meta-analysis of animal trials[J]. Resuscitation, 2012, 83(4): 417-422. DOI:10.1016/ j.resuscitation.2011.12.021.
[20] ICU-ROX Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group, Mackle D, Bellomo R, et al. Conservative oxygen therapy during mechanical ventilation in the ICU[J]. N Engl J Med, 2020, 382(11): 989-998. DOI:10.1056/ NEJMoa1903297.
[21] Roberts BW, Karagiannis P, Coletta M, et al. Effects of PaCO2 derangements on clinical outcomes after cerebral injury: A systematic review[J]. Resuscitation, 2015, 91: 32-41. DOI:10.1016/ j.resuscitation.2015.03.015.
[22] Hope Kilgannon J, Hunter BR, Puskarich MA, et al. Partial pressure of arterial carbon dioxide after resuscitation from cardiac arrest and neurological outcome: A prospective multi-center protocol-directed cohort study[J]. Resuscitation, 2019, 135: 212-220. DOI:10.1016/ j.resuscitation.2018.11.015.
[23] Wang HE, Prince DK, Drennan IR, et al. Post-resuscitation arterial oxygen and carbon dioxide and outcomes after out-of-hospital cardiac arrest[J]. Resuscitation, 2017, 120: 113-118. DOI:10.1016/ j.resuscitation.2017.08.244.
[24] Oksanen T, Skrifvars M, Wilkman E, et al. Postresuscitation hemodynamics during therapeutic hypothermia after out-ofhospital cardiac arrest with ventricular fibrillation: A retrospective study[J]. Resuscitation, 2014, 85(8): 1018-1024. DOI:10.1016/ j.resuscitation.2014.04.026.
[25] Cha KC, Kim HI, Kim OH, et al. Echocardiographic patterns of postresuscitation myocardial dysfunction[J]. Resuscitation, 2018, 124: 90-95. DOI:10.1016/j.resuscitation.2018.01.019.
[26] Anderson RJ, Jinadasa SP, Hsu L, et al. Shock subtypes by left ventricular ejection fraction following out-of-hospital cardiac arrest[J]. Crit Care, 2018, 22(1): 162. DOI:10.1186/s13054-018- 2078-x.
[27] Russo JJ, di Santo P, Simard T, et al. Optimal mean arterial pressure in comatose survivors of out-of-hospital cardiac arrest: An analysis of area below blood pressure thresholds[J]. Resuscitation, 2018, 128: 175-180. DOI:10.1016/j.resuscitation.2018.04.028.
[28] Kim YW, Cha KC, Cha YS, et al. Shock duration after resuscitation is associated with occurrence of post-cardiac arrest acute kidney injury[J]. J Korean Med Sci, 2015, 30(6): 802-807. DOI:10.3346/ jkms.2015.30.6.802.
[29] Grand J, Lilja G, Kjaergaard J, et al. Arterial blood pressure during targeted temperature management after out-of-hospital cardiac arrest and association with brain injury and long-term cognitive function[J]. Eur Heart J Acute Cardiovasc Care, 2020, 9(4_suppl): S122-S130. DOI:10.1177/2048872619860804.
[30] Riveiro DF, Oliveira VM, Braunner JS, et al. Evaluation of serum lactate, central venous saturation, and venous-arterial carbon dioxide difference in the prediction of mortality in postcardiac arrest syndrome[J]. J Intensive Care Med, 2016, 31(8): 544-552. DOI:10.1177/0885066615592865.
[31] Gamper G, Havel C, Arrich J, et al. Vasopressors for hypotensive shock[J]. Cochrane Database Syst Rev, 2016, 2: CD003709. DOI:10.1002/14651858.CD003709.pub4.
[32] Vasquez A, Kern KB, Hilwig RW, et al. Optimal dosing of dobutamine for treating post-resuscitation left ventricular dysfunction[J]. Resuscitation, 2004, 61(2): 199-207. DOI:10.1016/ j.resuscitation.2004.01.002.
[33] Janiczek JA, Winger DG, Coppler P, et al. Hemodynamic resuscitation characteristics associated with improved survival and shock resolution after cardiac arrest[J]. Shock, 2016, 45(6): 613-619. DOI:10.1097/SHK.0000000000000554.
[34] Ostenfeld S, Lindholm MG, Kjaergaard J, et al. Prognostic implication of out-of-hospital cardiac arrest in patients with cardiogenic shock and acute myocardial infarction[J]. Resuscitation, 2015, 87: 57-62. DOI:10.1016/j.resuscitation.2014.11.010.
[35] Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 esc guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European society of cardiology (esc). endorsed by: Association for European paediatric and congenital cardiology (aepc)[J]. Eur Heart J, 2015, 36(41): 2793- 2867. DOI:10.1093/eurheartj/ehv316.
[36] Bro-Jeppesen J, Johansson PI, Hassager C, et al. Endothelial activation/injury and associations with severity of post-cardiac arrest syndrome and mortality after out-of-hospital cardiac arrest[J]. Resuscitation, 2016, 107: 71-79. DOI:10.1016/ j.resuscitation.2016.08.006.
[37] Bro-Jeppesen J, Kjaergaard J, Wanscher M, et al. Systemic inflammatory response and potential prognostic implications after out-of-hospital cardiac arrest: A substudy of the target temperature management trial[J]. Crit Care Med, 2015, 43(6): 1223-1232. DOI:10.1097/CCM.0000000000000937.
[38] Nee J, Jörres A, Krannich A, et al. Elimination of glutamate using CRRT for 72 h in patients with post-cardiac arrest syndrome: A randomized clinical pilot trial[J]. Resuscitation, 2019, 144: 54-59. DOI:10.1016/j.resuscitation.2019.09.020.
[39] Lopez-de-Sa E, Juarez M, Armada E, et al. A multicentre randomized pilot trial on the effectiveness of different levels of cooling in comatose survivors of out-of-hospital cardiac arrest: The FROST-I trial[J]. Intensive Care Med, 2018, 44(11): 1807-1815. DOI:10.1007/ s00134-018-5256-z.
[40] Makker P, Kanei Y, Misra D. Clinical effffect of rebound hyperthermia after cooling postcardiac arrest: A meta-analysis[J]. Ther Hypothermia Temp Manag, 2017, 7(4): 206-209. DOI:10.1089/ther.2017.0009.
[41] Gupta HV, Caviness JN. Post-hypoxic myoclonus: Current concepts, neurophysiology, and treatment[J]. Tremor Other Hyperkinet Mov (N Y), 2016, 6: 409. DOI:10.7916/D89C6XM4.
[42] Aicua Rapun I, Novy J, Solari D, et al. Early Lance-Adams syndrome after cardiac arrest: Prevalence, time to return to awareness, and outcome in a large cohort[J]. Resuscitation, 2017, 115: 169-172. DOI:10.1016/j.resuscitation.2017.03.020.
[43] Shao F, Li CS, Liang LR, et al. Outcome of out-of-hospital cardiac arrests in Beijing, China[J]. Resuscitation, 2014, 85(11): 1411-1417. DOI:10.1016/j.resuscitation.2014.08.008.
[44] Yannopoulos D, Bartos JA, Aufderheide TP, et al. The evolving role of the cardiac catheterization laboratory in the management of patients with out-of-hospital cardiac arrest: A scientific statement from the American Heart Association[J]. Circulation, 2019, 139(12): e530-e552. DOI:10.1161/CIR.0000000000000630.
[45] Kern KB, Lotun K, Patel N, et al. Outcomes of comatose cardiac arrest survivors with and without ST-segment elevation myocardial infarction: importance of coronary angiography[J]. JACC Cardiovasc Interv, 2015, 8(8): 1031-1040. DOI:10.1016/j.jcin.2015.02.021.
[46] Geri G, Dumas F, Bougouin W, et al. Immediate percutaneous coronary intervention is associated with improved shortand long-term survival after out-of-hospital cardiac arrest[J]. Circ Cardiovasc Interv, 2015, 8(10): e002303. DOI:10.1161/ circinterventions.114.002303.
[47] Elfwén L, Lagedal R, James S, et al. Coronary angiography in outof-hospital cardiac arrest without ST elevation on ECG-Short- and long-term survival[J]. Am Heart J, 2018, 200: 90-95. DOI:10.1016/ j.ahj.2018.03.009.
[48] Lemiale V, Dumas F, Mongardon N, et al. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort[J]. Intensive Care Med, 2013, 39(11): 1972-1980. DOI:10.1007/s00134-013-3043-4.
[49] Sandroni C, Cariou A, Cavallaro F, et al. Prognostication in comatose survivors of cardiac arrest: an advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine[J]. Resuscitation, 2014, 85(12): 1779-1789. DOI:10.1016/ j.resuscitation.2014.08.011.
[50] Wilder Schaaf KP, Artman LK, Peberdy MA, et al. Anxiety, depression, and PTSD following cardiac arrest: A systematic review of the literature[J]. Resuscitation, 2013, 84(7): 873-877. DOI:10.1016/j.resuscitation.2012.11.021.
[51] Presciutti A, Verma J, Pavol M, et al. Posttraumatic stress and depressive symptoms characterize cardiac arrest survivors' perceived recovery at hospital discharge[J]. Gen Hosp Psychiatry, 2018, 53: 108-113. DOI:10.1016/j.genhosppsych.2018.02.006.
[52] Presciutti A, Sobczak E, Sumner JA, et al. The impact of psychological distress on long-term recovery perceptions in survivors of cardiac arrest[J]. J Crit Care, 2019, 50: 227-233. DOI:10.1016/ j.jcrc.2018.12.011.
[53] Lilja G, Nilsson G, Nielsen N, et al. Anxiety and depression among out-of-hospital cardiac arrest survivors[J]. Resuscitation, 2015, 97:6875.DOI:10.1016/j.resuscitation.2015.09.389.