科研进展
【文献导读】多中心协作预防小儿心脏重症监护室内的心脏骤停
Preventing Cardiac Arrest in the Pediatric Cardiac Intensive Care Unit Through Multicenter Collaboration
多中心协作预防小儿心脏重症监护室内的心脏骤停
翻译:桑文涛、IE-learning平台翻译团队
IMPORTANCE
Preventing in-hospital cardiac arrest (IHCA) likely represents an effective strategy to improve outcomes for critically ill patients, but feasibility of IHCA prevention remains unclear.
重要性
预防院内心脏骤停 (IHCA) 可能是改善重症患者预后的有效策略,但 预防IHCA的可行性仍不清楚。
OBJECTIVE
To determine whether a low-technology cardiac arrest prevention (CAP) practice bundle decreases IHCA rate.
目的
确定低技术水平的心脏骤停预防 (CAP) 集束化管理策略是否会降低 IHCA 发生率。
DESIGN, SETTING, AND PARTICIPANTS
Pediatric cardiac intensive care unit (CICU) teams from the Pediatric Cardiac Critical Care Consortium (PC4) formed a collaborative learning network to implement the CAP bundle consistent with the Institute for Healthcare Improvement framework; 15 hospitals implemented the bundle voluntarily. Risk-adjusted IHCA incidence rates were analyzed across 2 time periods, 12 months (baseline) and 18 months after CAP implementation (intervention) using difference-in-differences (DID) regression to compare 15 CAP and 16 control PC4 hospitals that chose not to participate in CAP but had IHCA rates tracked in the PC4 registry. Patients deemed at high risk for IHCA, based on a priori evidence-based criteria and empirical hospital-specific criteria, were selected to receive the CAP bundle. Data were collected from July 2018 to December 2019, and data were analyzed from March to August 2020.
设计、参与单位和纳入人群
来自儿科心脏重症监护联盟 (PC4) 的儿科心脏重症监护室 (CICU) 团队组成了一个协作学习网络,实施符合医疗保健改进研究所框架制定的CAP集束化管理策略;15家医院自愿实施集束化管理策略。在CAP 实施后12个月(基线)和18个月(干预)的两个时间段使用双重差分法(DID) 回归比较分析了15家实施CAP集束化管理策略的医院和16家对照PC4医院风险调整后的 IHCA 发病率,对照组医院选择不实施 CAP集束化管理策略,但在 PC4登记中跟踪IHCA发生率。根据先验循证标准和经验性医院特定标准,被认为具有IHCA高风险的患者被选择接受CAP集束化管理策略。数据收集时间为 2018 年7月至 2019 年12月,数据分析时间为2020年3月至2020 年8月。
INTERVENTIONS
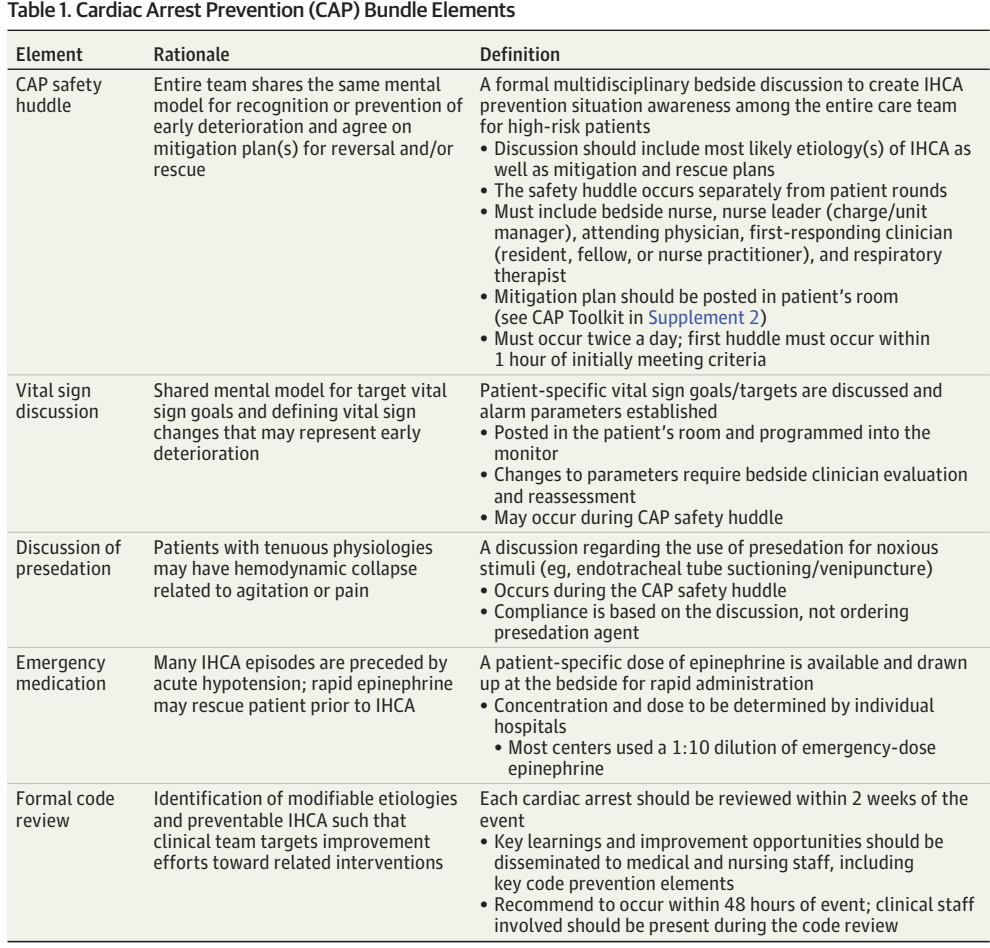
CAP bundle included 5 elements developed to promote increased situational awareness and communication among bedside clinicians to recognize and mitigate deterioration in high-risk patients.
干预
CAP集束化管理策略包括5个元素,旨在促进床边临床医生提高情景意识和沟通,以识别和缓解高危患者的恶化。
MAIN OUTCOMES AND MEASURES
Risk-adjusted IHCA incidence rate across all CICU admissions (IHCA events divided by all admissions).
主要结果和措施
所有CICU入院患者的风险调整后IHCA发病率(IHCA事件除以所有入院患者)。
RESULTS
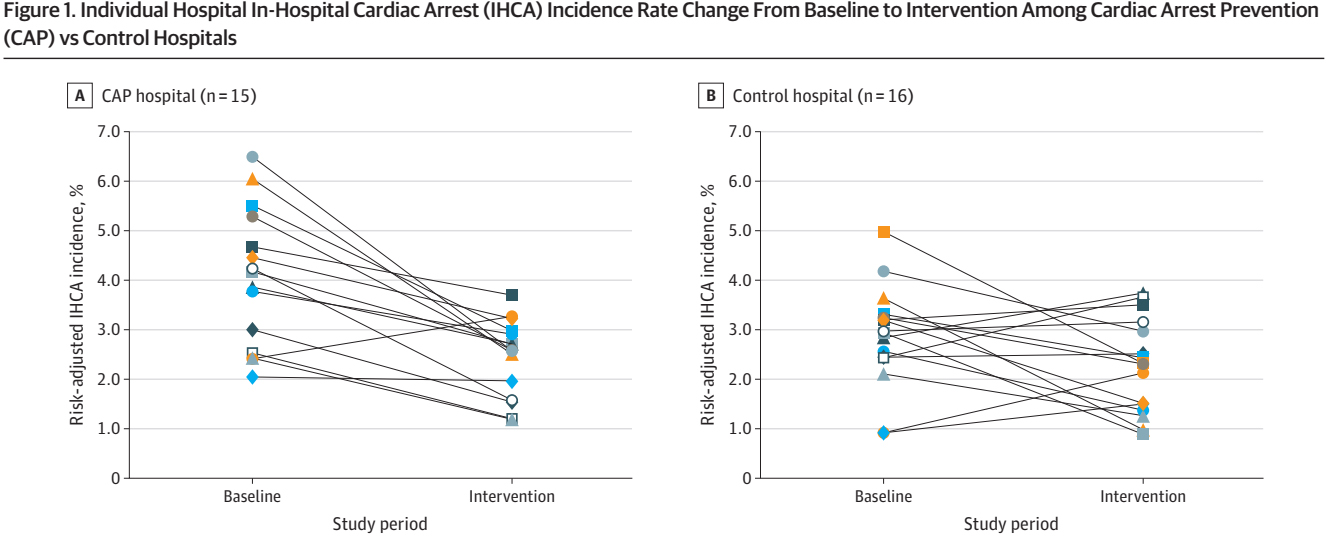
The bundle was activated in 2664 of 10 510 CAP hospital admissions (25.3%); admission characteristics were similar across study periods. There was a 30% relative reduction in risk-adjusted IHCA incidence rate at CAP hospitals (intervention period: 2.6%; 95% CI, 2.2-2.9; baseline: 3.7%; 95% CI, 3.1-4.0), but no change at control hospitals (intervention period: 2.7%; 95% CI, 2.3-2.9; baseline: 2.7%; 95% CI, 2.2-3.0). DID analysis confirmed significantly reduced odds of IHCA among all admissions at CAP hospitals compared with control hospitals during the intervention period vs baseline (odds ratio, 0.72; 95% CI, 0.56-0.91; P = .01). DID odds ratios were 0.72 (95% CI, 0.53-0.98) for the surgical subgroup, 0.74 (95% CI, 0.48-1.14) for the medical subgroup, and 0.72 (95% CI, 0.50-1.03) for the high-risk admission subgroup at CAP hospitals after intervention. All-cause risk-adjusted mortality rate did not change after intervention.
结果
在10510例CAP住院患者中有2664例激活了集束化管理策略(25.3%);不同研究时期的入院特征相似。CAP医院经风险调整后的IHCA发病率相对降低了30%(干预期:2.6%;95% CI,2.2-2.9;基线:3.7%;95% CI,3.1-4.0),但在对照医院无变化(干预期:2.7%;95% CI,2.3-2.9;基线:2.7%;95% CI,2.2-3.0)。 DID 分析证实,在干预期间,与对照组医院相比,CAP医院所有入院患者发生IHCA的可能性显著降低(优势比,0.72;95% CI,0.56-0.91;P =0.01)。在CAP医院中,进行干预后,手术组、内科组和入院时高风险组的DID优势比分别为0.72(95%CI,0.53-0.98)、0.74(95%CI,0.48-1.14)和0.72(95%CI,0.50-1.03)。干预后全因风险调整死亡率没有变化。


CONCLUSIONS AND RELEVANCE
Implementation of this CAP bundle led to significant IHCA reduction across multiple pediatric CICUs. Future studies may determine if this bundle can be effective in other critically ill populations.
结论和相关性
该CAP集束化管理策略的实施显著减少了多个儿科CICU的IHCA发生率。未来的研究可能会确定这种方法对其他危重人群是否有效。
原文链接:https://jamanetwork.com/journals/jamapediatrics/article-abstract/2793938?resultClick=1