科研进展
【文献导读】The New England Journal of Medicine:血小板减少患者置入CVC前输注血小板的研究
Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia.
血小板减少患者置入CVC前输注血小板的研究
文章来源:N Engl J Med 2023;388:1956-65. DOI: 10.1056/NEJMoa2214322
编译:张健,IE-learning翻译团队
Background
The Transfusion guidelines regarding platelet-count thresholds before the placement of a central venous catheter (CVC) offer conflicting recommendations because of a lack of good-quality evidence. The routine use of ultrasound guidance has decreased CVC-related bleeding complications.
研究背景
由于缺乏高质量证据,关于放置中心静脉导管(CVC)前的血小板计数阈值的输血指南提出了相互矛盾的建议。超声引导置管的常规应用降低了CVC相关出血并发症。
Methods
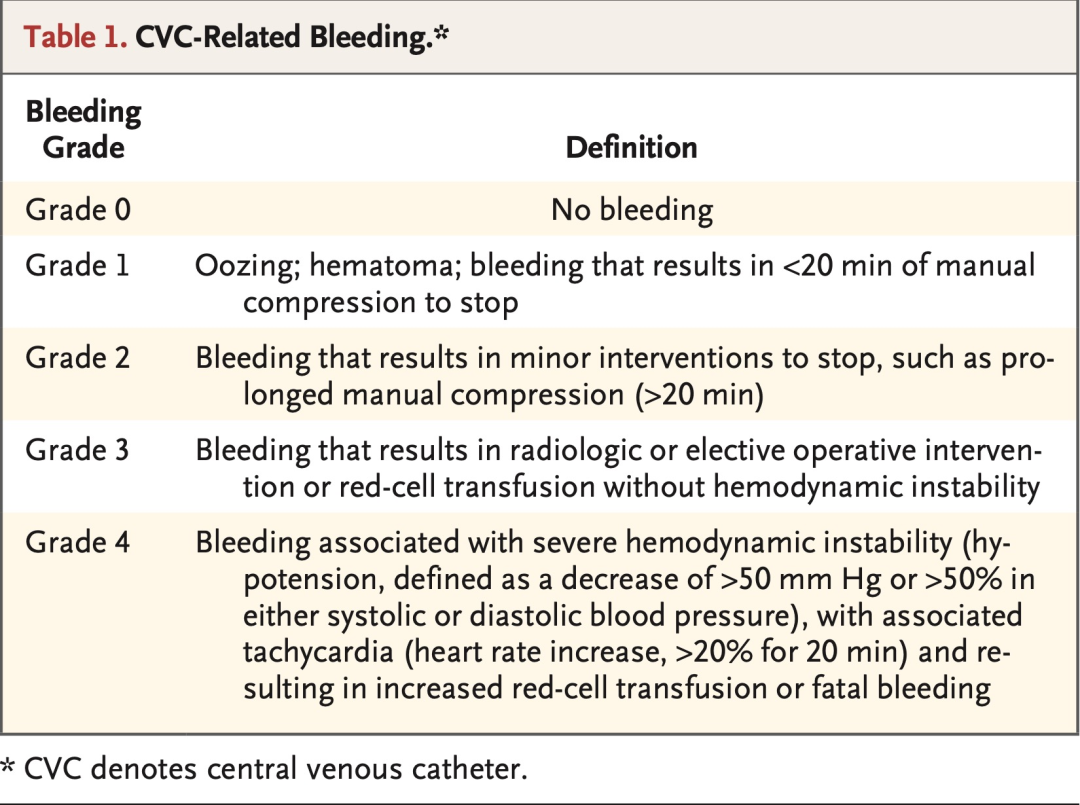
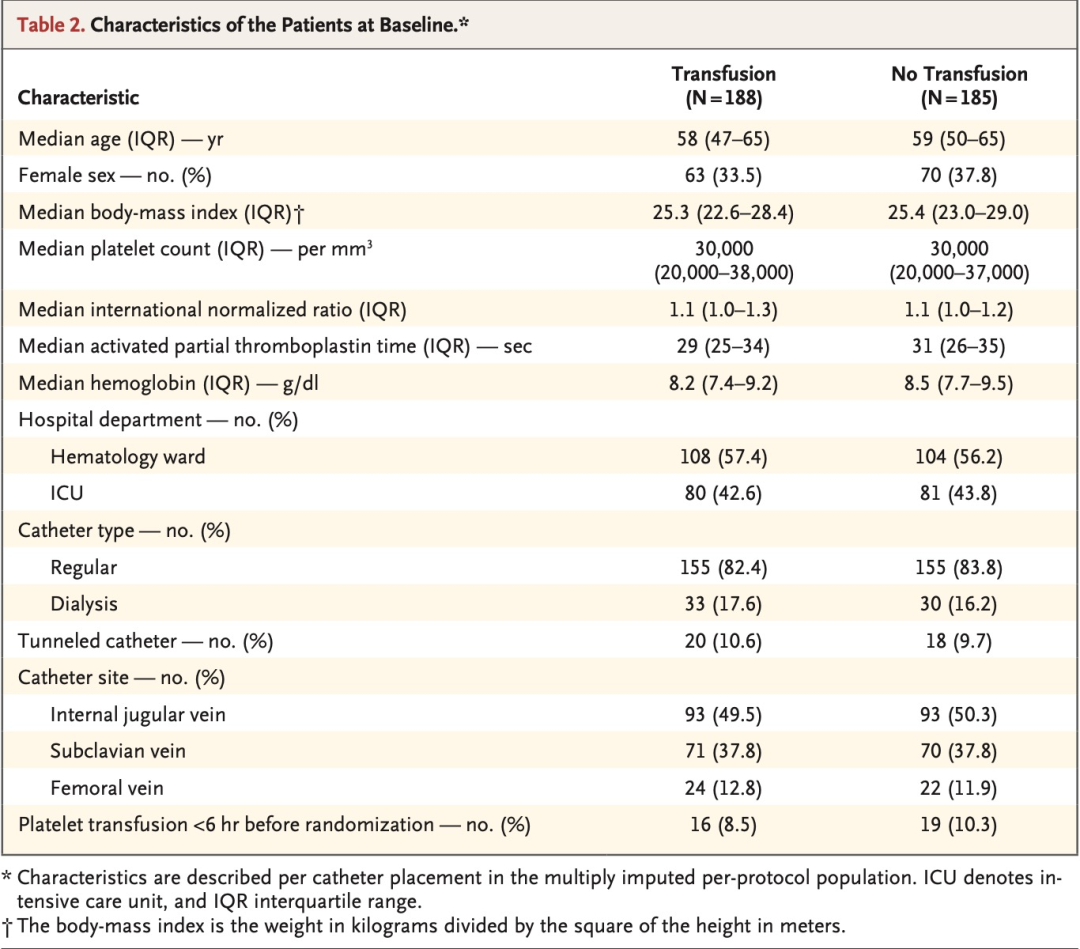
In a multicenter, randomized, controlled, noninferiority trial, we randomly assigned patients with severe thrombocytopenia who were being treated on the hematology ward or in the intensive care unit to receive either one unit of prophylactic platelet transfusion or no platelet transfusion before ultrasound-guided CVC placement. All CVC placement procedures involving patients with thrombocytopenia who had a platelet count of 10,000 to 50,000 per cubic millimeter within 24 hours before the procedure were eligible for inclusion. CVCs were required to be in place for at least 24 hours. Exclusion criteria were the use of a therapeutically administered anticoagulant, a history of congenital or acquired coagulation factor deficiency or bleeding risk, or a spontaneously prolonged international normalized ratio (INR) of 1.5 or more. Patients were randomly assigned in a 1:1 ratio to receive either one unit of platelet concentrate or no platelet transfusion before CVC placement. The primary outcome was the occurrence of catheter-related bleeding of grade 2 to 4 within 24 hours after CVC placement. A key secondary outcome was major (grade 3 or 4) bleeding. Other secondary outcomes were grade 1 bleeding, platelet and red-cell transfusions within 24 hours after CVC placement, hemoglobin level and platelet count at 1 hour and 24 hours after CVC placement, allergic transfusion reaction within 24 hours after CVC placement, the onset of acute lung injury within 48 hours after CVC placement, the length of ICU and hospital stay, in-hospital mortality, and financial costs. The noninferiority margin was an upper boundary of the 90% confidence interval of 3.5 for the relative risk.
方法
在一项多中心、随机、对照、非劣效性试验中,我们将在血液科病房或重症监护病房接受治疗的重度血小板减少患者进行随机分组,分别在超声引导置入CVC前接受1个单位的预防性血小板输注或不接受血小板输注。所有接受CVC置入操作的血小板减少患者要求术前24小时内血小板计数为10,000 ~ 50,000/ml方符合纳入标准。CVC要求至少留置24小时。排除标准包括治疗性使用抗凝剂,有先天性或获得性凝血因子缺乏或出血风险的病史,或自发延长的国际标准化比值(INR)≥1.5。 患者按照1:1的比例随机分组,分别在置入CVC前接受1个单位的浓缩血小板输注或不输注血小板。主要结局是CVC置入后24小时内发生2~4级导管相关出血。关键次要结局是导管相关大出血(3级或4级)。其他次要结局包括1级出血、CVC置入后24 h内血小板和红细胞输注量、CVC置入1h后和24h后血红蛋白水平和血小板计数、CVC置入后24h内过敏性输血反应、CVC置入后48 h内发生急性肺损伤、ICU入住时间和住院时间、住院病死率和经济费用。非劣效性界值是相对危险度的90%置信区间的上限3.5。
Results:
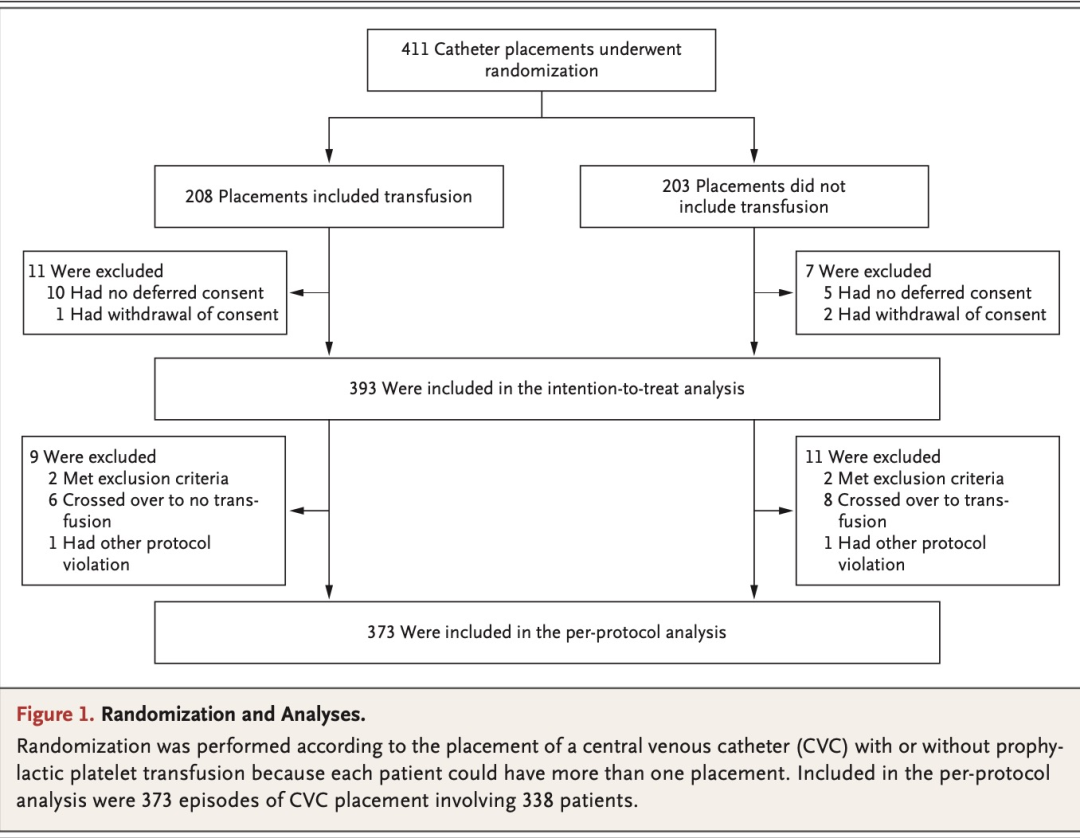
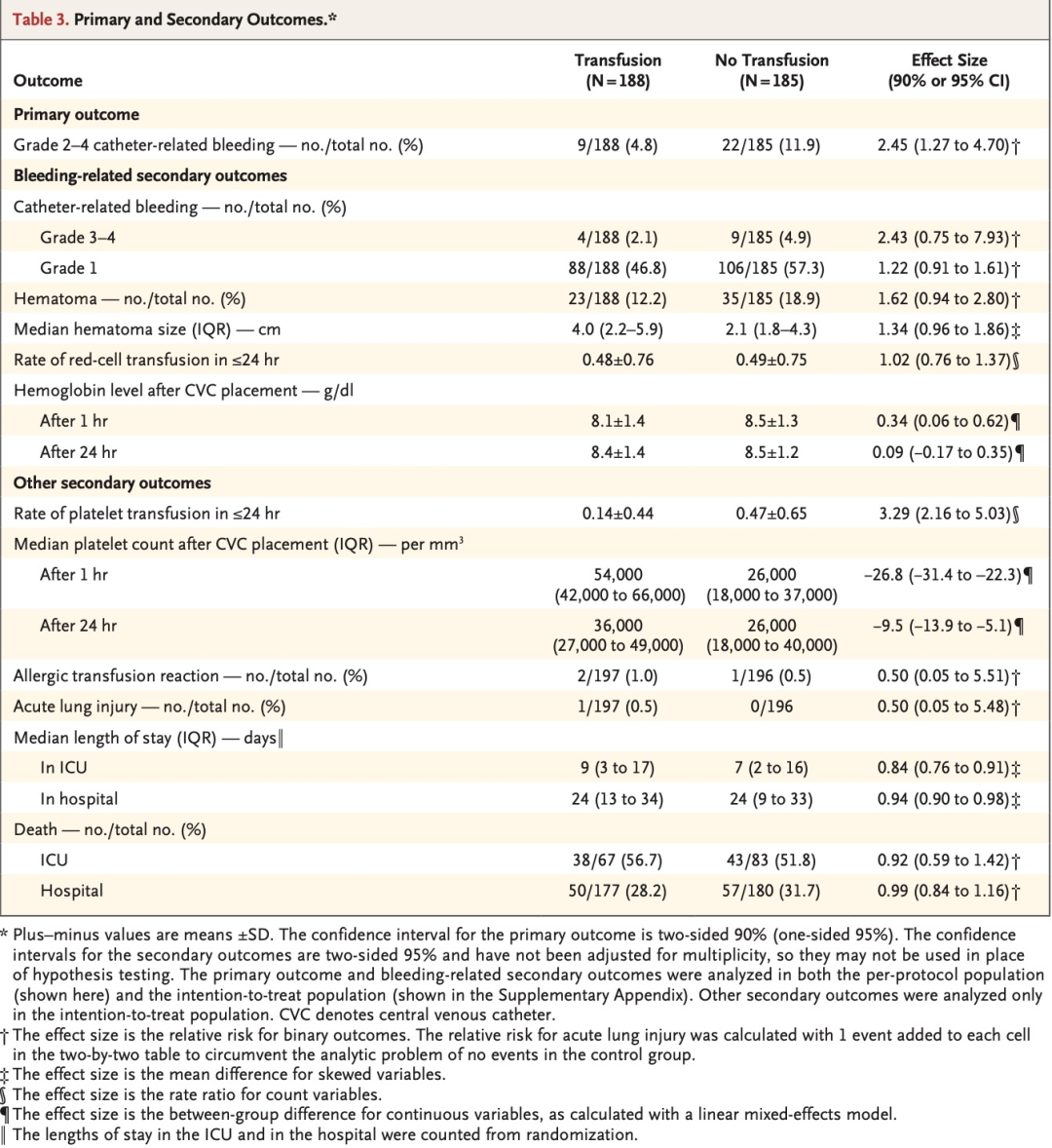
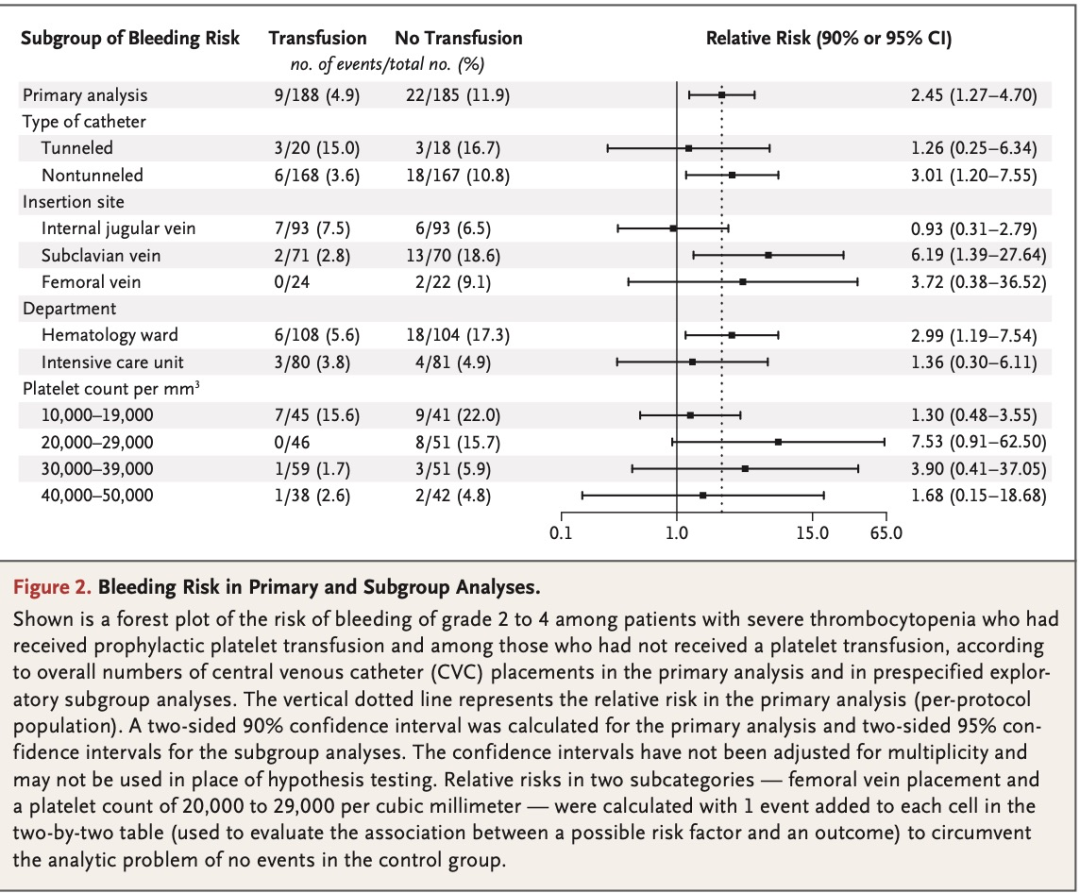
We included 373 episodes of CVC placement involving 338 patients in the perprotocol primary analysis. Catheter-related bleeding of grade 2 to 4 occurred in 9 of 188 patients (4.8%) in the transfusion group and in 22 of 185 patients (11.9%) in the no-transfusion group (relative risk, 2.45; 90% confidence interval [CI], 1.27 to 4.70). Catheter-related bleeding of grade 3 or 4 occurred in 4 of 188 patients (2.1%) in the transfusion group and in 9 of 185 patients (4.9%) in the no-transfusion group (relative risk, 2.43; 95% CI, 0.75 to 7.93). A total of 15 adverse events were observed; of these events, 13 (all grade 3 catheter-related bleeding [4 in the transfusion group and 9 in the no-transfusion group]) were categorized as serious. The net savings of withholding prophylactic platelet transfusion before CVC placement was $410 per catheter placement.
结果
在符合方案的主要分析中,我们共纳入了338例患者的373次CVC置入。输血组188例患者中的9例(4.8%)和未输血组185例患者中的22例(11.9%)发生了2~4级导管相关性出血(相对危险度 2.45;90%置信区间[CI],1.27~4.70)。输血组188例患者中的4例(2.1%)和未输血组185例患者中的9例(4.9%)发生了3级或4级导管相关出血(相对危险度 2.43;95% CI, 0.75~7.93)。本研究共观察到15起不良事件。在这些事件中,13起(均为3级导管相关出血 [输血组4起,未输血组9起])被归类为严重事件。在置入CVC前不进行预防性血小板输注可为每次置入CVC净节省410美元。
Discussion
Despite our overall findings regarding CVC-related bleeding complications in all patients with a platelet count of 10,000~50,000/ml, we would advocate for a more personalized approath. We would consider prophylactic platelet transfusion in patients with a platelet count of less than 30,000/ml, especially on the hematology ward, because these patients are likely to require a platelet transfusion within 24 hours anyway. For patients in the ICU with lower platelet counts, we would consider a no-transfusion strategy with intensive monitoring and a low threshold for the therapeutic use of blood products. The patients in the ICU had a lower bleeding risk than those on the hematology ward, and the ICU setting allows for more intensive monitoring. We would consider raising platelet-count thresholds for tunneled catheter insertion as opposed to nontunneled catheter insertion, because the bleeding risk associated with tunneled catheters was considerably higher. Finally, we would consider performing a follow-up trial to investigate the prophylactic transfusion of multiple units of platelet concentrate in patients with a platelet count of less than 20,000/ml, because their bleeding risk remained high even after one unit of platelets.
讨论
尽管我们在血小板计数为10,000~50,000/ml的所有患者中发现了CVC相关出血并发症的总体结果,但我们主张采用更个体化的治疗方法。我们考虑对血小板计数低于30,000/ml的患者进行预防性血小板输注,尤其是在血液科病房,因为这些患者无论如何都可能需要在24小时内输注血小板。对于住在ICU的血小板计数较低的患者,我们将考虑暂不输血的策略,并进行密切监测,且将血液制品的治疗性使用阈值设为更低。因为与血液科患者相比,ICU患者的出血风险较低,而且ICU可以进行更严密的监测。我们将考虑提高经隧道导管置入的血小板计数阈值,而不是非经隧道导管置入的血小板计数阈值,原因是与隧道导管相关的出血风险显著较高。最后,我们将考虑开展一项随访试验,研究在血小板计数低于20,000/ml的患者中预防性输注多个单位的浓缩血小板,因为即使在输注1个单位血小板后,出血风险仍然很高。
Conclusions
The withholding of prophylactic platelet transfusion before CVC placement in patients with a platelet count of 10,000 to 50,000 per cubic millimeter did not meet the predefined margin for noninferiority and resulted in more CVC-related bleeding events than prophylactic platelet transfusion.
结论
在血小板计数为10,000~50,000/ml的患者中,CVC置入前不给予预防性血小板输注未达到预设的非劣效性界值,并且导致了比给予预防性血小板输注更多的CVC相关出血事件。
编辑丨国康
审核丨边圆 徐峰
IE-Learning急危重症学习平台
原创声明:文章权限归原作者所有,如需转载请联系我平台。