科研进展
【文献导读】Circulation:心力衰竭患者的临床特征和转归:左心室射血分数是否存在阈值和拐点并作为临床分类的依据?
Clinical Characteristics and Outcomes in Patients With Heart Failure: Are There Thresholds and Inflection Points in Left Ventricular Ejection Fraction and Thresholds Justifying a Clinical Classification?
Circulation:心力衰竭患者的临床特征和转归:左心室射血分数是否存在阈值和拐点并作为临床分类的依据?
文章来源:10.1161/CIRCULATIONAHA.122.063642
编译:杨威,IE-learning翻译团队
Background
Recent guidelines proposed a classification for heart failure (HF) on the basis of left ventricular ejection fraction (LVEF), although it remains unclear whether the divisions chosen were biologically rational. Using patients spanning the full range of LVEF, we examined whether there was evidence of LVEF thresholds in patient characteristics or inflection points in clinical outcomes.
背景
最近的指南建议以左室射血分数(LVEF)为基础对心力衰竭(HF)进行分类,尽管目前尚不清楚所选择的分区是否具有生物学合理性。使用横跨整个LVEF范围的患者,我们检查了患者特征中是否存在LVEF阈值的证据,或者临床结果中是否存在拐点。
Methods
Using patient-level information, we created a merged dataset of 33699 participants who had been enrolled in 6 randomized controlled HF trials including patients with reduced and preserved ejection fraction. The relationship between the incidence of allcause death (and specific causes of death) and HF hospitalization, and LVEF, was evaluated using Poisson regression models.
利用患者水平的信息,我们创建了一个合并的数据集,其中包括33699名参与者,他们参加了6项随机对照心力衰竭试验[CHAME(坎地沙坦在心力衰竭降低死亡率和发病率评估中的作用)、I-PREVISE(伊贝沙坦治疗收缩功能保留的心力衰竭)、PAGAMUM-HF(ARNI与ACEI的前瞻性比较以确定对全球心力衰竭死亡率和发病率的影响)、TOPCAT(美洲;ARNI与ARB对射血分数保留的心衰患者的治疗效果的前瞻性比较)、AMERAGE(Aliskiren试验将心力衰竭患者的预后降至最低)和PARAGON-HF(ARNI与ARB的前瞻性比较射血分数保留的心衰患者的全球结果)],其中包括射血分数降低和保留的患者。使用Poisson回归模型评估全死因死亡(和特定死因)与心力衰竭住院时间和左心室射血分数之间的关系。
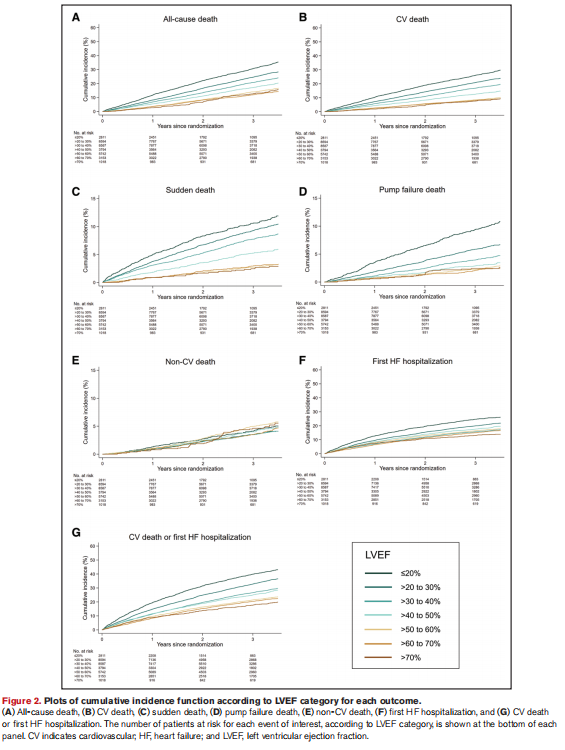
全因死亡率,这是最客观也是最重要的结果,作为主要终点。我们还分析了非心血管死亡和心血管死亡,其中心血管死亡的两种主要模式,即猝死和泵衰竭死亡、第一次心衰住院、心血管死亡或首次心力衰竭住院、心力衰竭总住院(首次和复发)、心血管死亡和心力衰竭总住院的综合情况。
Results
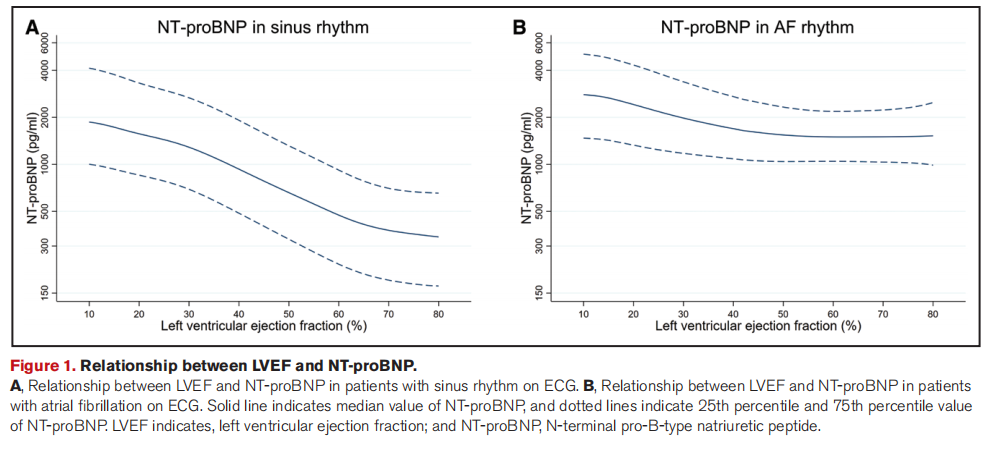
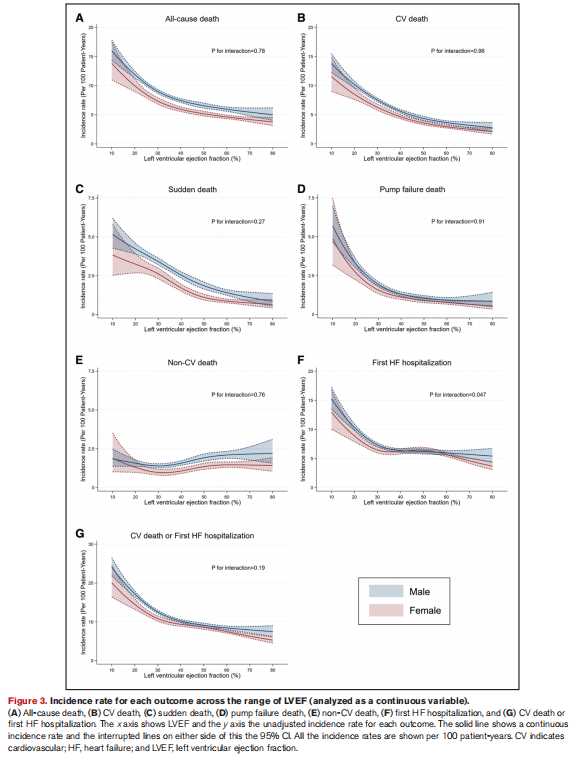
As LVEF increased, age, the proportion of women, body mass index, systolic blood pressure, and prevalence of atrial fibrillation and diabetes increased, whereas ischemic pathogenesis, estimated glomerular filtration rate, and NT-proBNP (N-terminal pro-B-type natriuretic peptide) decreased. As LVEF increased >50%, age and the proportion of women continued to increase, and ischemic pathogenesis and NT-proBNP decreased, but other characteristics did not change meaningfully. The incidence of most clinical outcomes (except noncardiovascular death) decreased as LVEF increased, with a LVEF inflection point of around 50% for all-cause death and cardiovascular death, around 40% for pump failure death, and around 35% for HF hospitalization. Higher than those thresholds, there was little further decline in the incidence rate. There was no evidence of a J-shaped relationship between LVEF and death; no evidence of worse outcomes in patients with high-normal (“supranormal”) LVEF. Similarly, in a subset of patients with echocardiographic data, there were no structural differences in patients with a high-normal LVEF suggestive of amyloidosis, and NT-proBNP levels were consistent with this conclusion.
随着LVEF的增加,年龄、女性比例、体重指数、收缩压、心房颤动和糖尿病的患病率增加,而缺血发病机制、估计的肾小球滤过率和NT-ProBNP(N-末端前-B型利钠肽)减少。当LVEF增加>50%时,年龄和女性比例继续增加,缺血发病机制和NT-proBNP减少,但其他特征无明显变化。
大多数临床结果(非心血管死亡除外)的发生率随着LVEF的增加而下降,全因死亡和心血管死亡的LVEF拐点约为50%,泵衰竭死亡约为40%,心力衰竭住院约为35%。高于这些阈值,发病率几乎没有进一步下降。没有证据表明左心室射血分数和死亡之间存在J型关系;没有证据表明左心室射血分数高(“超常”)的患者的预后更差。类似地,在超声心动图数据的一部分患者中,LVEF正常值高的患者没有结构性差异,提示淀粉样变性,NT-proBNP水平与这一结论一致。
Conclusions:
In patients with HF, there was a LVEF threshold of around 40% to 50% where the pattern of patient characteristics changed, and event rates began to increase compared with higher LVEF values. Our findings provide evidence to support current upper LVEF thresholds defining HF with mildly reduced ejection fraction on the basis of prognosis.
在心力衰竭患者中,有一个大约40%到50%的LVEF阈值,在那里患者的特征模式发生了变化,与较高的LVEF值相比,事件发生率开始增加。我们的发现提供了证据,支持目前的LVEF上限阈值根据预后来定义射血分数轻度降低的心衰。
编辑丨国康
审核丨边圆 徐峰
IE-Learning急危重症学习平台
原创声明:文章权限归原作者所有,如需转载请联系我平台。